
Health system leaders are navigating an era of rising performance expectations, tightening margins, and increasing clinical complexity. Most improvement efforts fall short not because of poor intent — but because they fail to reach the actual moment of clinical decision-making.
Articles are written for senior clinical, quality, and operational leaders navigating real tradeoffs. Content is organized around where decisions break down and where the industry is heading — not theoretical models — to support both strategic reflection and practical application.
Some Examples of What You’ll Find Here
Clinical quality, patient safety, and health system performance
Analysis of clinical variation and reliability
Governance models for clinical content and pathways
Responsible use of AI in healthcare operations
Operational lessons from health system improvement efforts
View Our Insights Here from the Field
Written for healthcare leaders responsible for clinical excellence, quality, safety, and enterprise performance — with an emphasis on clarity, structural understanding, and practical implications rather than abstract commentary.
Protocol Debt: The Clinical Liability That Isn't on Your Balance Sheet
Most health systems have no reliable way to track how outdated their clinical guidelines have become. This is protocol debt — and it's accruing faster than ever.
Most health systems cannot systematically identify which clinical guidelines are outdated — creating invisible compliance exposure and clinical variation that compounds over time.
Protocol debt doesn't just accumulate slowly — AI adoption is accelerating it, surfacing unvalidated guidance that conflicts with unmaintained institutional standards.
The fix isn't better storage — it's governance infrastructure that treats clinical content like code: with version control, review cycles, deprecation policies, and clear ownership.

Shadow AI in Healthcare: What the Numbers Reveal About the Adoption Arc We’re On
When clinicians bypass approved channels to use unauthorized AI, the story isn’t rogue behavior. It’s a diffusion curve healthcare leadership is not yet governing.
20% of clinicians use unauthorized AI — and 40% more know colleagues who do
Healthcare has crossed the chasm on documentation AI — the clinical chasm is what remains
The answer to shadow AI isn't enforcement — it's closing the gap between what clinicians can access informally and what institutions can govern
What Health Systems Get Wrong About Clinical AI (And What the Good Ones Do Differently)
AI can accelerate clinical decision support. It cannot replace the governance infrastructure it runs on.
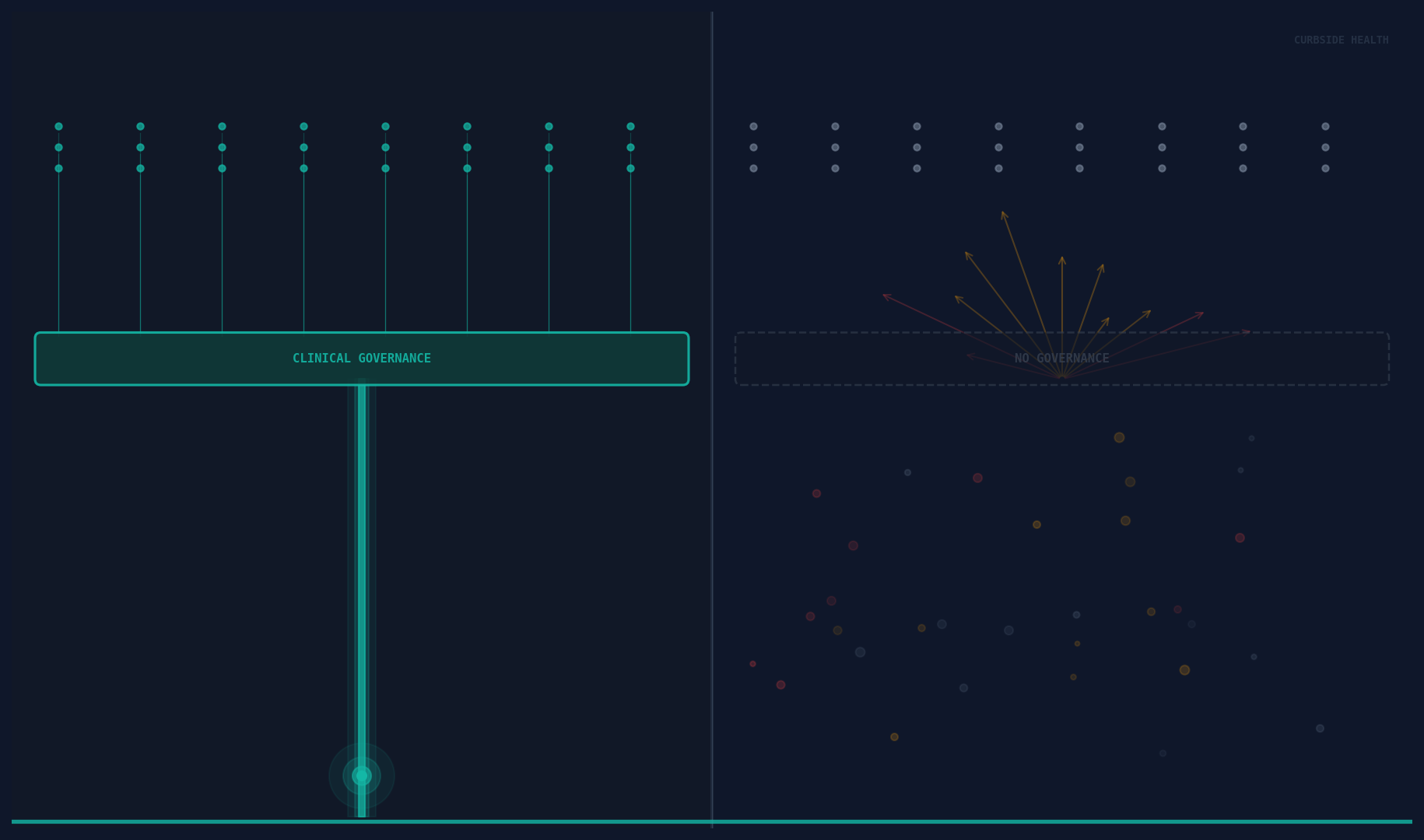
AI without local governance produces generic recommendations clinicians learn to bypass
The failure mode is almost never the algorithm — it’s the absent governance layer underneath it
Systems winning on clinical AI build content governance before or in parallel with AI deployment
The Utilization Gap: Why Pathways Gather Dust Instead of Driving Decisions
With the right tools, building pathways is no longer the bottleneck. Getting clinicians to actually use them is.
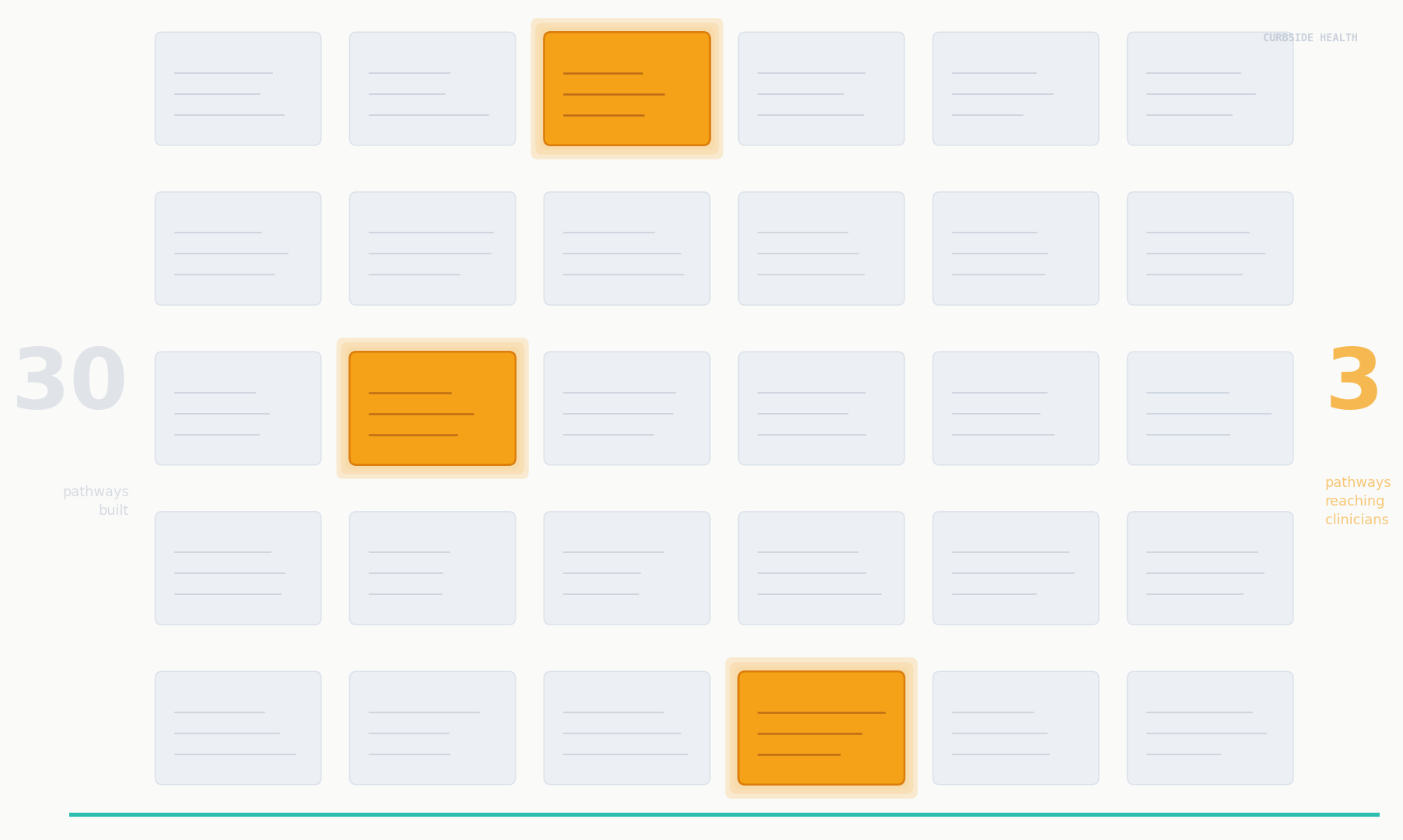
A pathway that isn’t used is a document, not a tool — value accrues from utilization, not existence
Pathways fail due to location, timing, currency, and awareness — infrastructure failures, not documentation failures
Closing the gap requires EHR integration, clinician awareness infrastructure, and utilization measurement
Clear Thinking for Complex Clinical Systems
Medicine is complex. That’s not a reason to stop standardizing.
Complexity isn't an argument against standardization — it demands better-designed standards
High-variation systems consistently underperform on quality, safety, and cost
Good governance accommodates clinical judgment while eliminating unwarranted variation

Why Clinical Variation Is Expensive — and Why Most Organizations Underestimate the Cost
The true price of unwarranted variation isn't on any dashboard. Here's why health systems keep getting the number wrong — and what it costs them to stay underinformed.
Claims data captures only output costs — the true burden includes physician cognitive load, regulatory exposure, and pathway abandonment
Most health systems underestimate variation costs by 2–3x, driving systematic under-investment in clinical governance
Pathway existence is not pathway utilization — ROI on clinical standardization lives in governance infrastructure, not the content alone

How to Use These Insights

Inform executive and board discussions
Support clinical and quality strategy development
Align improvement initiatives with CMS priorities
Provide shared language across leadership teams
Select updates and announcements may appear alongside thought leadership when relevant to platform evolution, partnerships, or industry context.
Clinical pathways that actually work.
© 2026 Curbside Health. All rights reserved.